#emergency-healthcare-funding
#emergency-healthcare-funding
[ follow ]
#healthcare #healthcare-access #patient-care #emergency-services #nhs #mental-health #public-safety #homelessness




Online Community Development
fromNextgov.com
2 weeks agoWhen disaster strikes, census data can help show who is in harm's way
The U.S. Census Bureau's OnTheMap for Emergency Management tool helps officials quickly estimate population and workforce data in disaster-affected areas to guide emergency response and recovery efforts.
fromwww.cbc.ca
3 days agoOffice space for emergency care: East-end Toronto hospital says patient demand is more than double capacity | CBC News
The emergency department at Michael Garron Hospital was built to care for about 150 patients a day, but now sees more than 300 patients daily, amounting to about 107,000 patients last year in a space designed for 50,000 annually.
Healthcare
Public health
fromwww.theguardian.com
3 weeks agoPatients face long journeys for medicines as pharmacies cut weekend hours
One in six English pharmacies have reduced weekend hours since 2022, causing over 20% loss of weekend opening hours and forcing patients to travel long distances or seek emergency care.
Social justice
fromwww.mercurynews.com
1 month agoLetters: Police are the wrong people for crisis intervention
Police lack the advanced clinical training and education of counselors and are inappropriate for crisis intervention; behavioral health-led responses by clinicians and social workers are more effective and cost-effective alternatives.
fromThe Nation
3 weeks agoA Motto for All Health Workers: Resist, Resist, Resist
What are scientists, clinicians, and public health practitioners supposed to do in this moment? What use is research when our patients might be deported tomorrow? Why try to stem the tide of outbreaks when the world has fallen apart? This is why: because even in these times, enlarging the scope of human knowledge matters. The search for cures still matters. The fate of individual patients still matters.
Public health


Information security
fromThe Hacker News
1 month agoTop 5 Ways Broken Triage Increases Business Risk Instead of Reducing It
Triage failures occur when decisions are made without execution evidence, causing false positives, missed threats, and higher costs; interactive sandboxes enable evidence-backed verdicts within seconds.
fromLos Angeles Times
1 month agoThere were 13 full-service public health clinics in L.A. County. Now there are 6
Because of budget cuts, the Los Angeles County Department of Public Health has ended clinical services at seven of its public health clinic sites. As of Feb. 27, the county is no longer providing services such as vaccinations, sexually transmitted infection testing and treatment, or tuberculosis diagnosis and specialty TB care at the affected locations, according to county officials and a department fact sheet.
Public health
fromNextgov.com
5 days agoHHS reverses Biden-era restructuring of its IT and tech operations
HHS Chief Information Officer Clark Minor stated that consolidating the CTO, CDO, and CAIO roles within his office allows the department to move faster on shared platforms and protect systems more effectively.
Healthcare
Mental health
fromBusiness Matters
1 month agoWhat Capitol City Residential Health Care Learned from Preventable Crises
Prevention-first, operations-focused residential care stabilizes high-acuity individuals by detecting missed signals, using consistent staffing, frequent plan reviews, and measured, person-centred adjustments.
fromLos Angeles Times
2 months agoHealthcare experts warn 'people will die' unless state steps up amid federal cuts
Federal cuts could strip about 1.2 million Californians of Medi-Cal coverage, with health experts warning the consequences could be dire. New work requirements and eligibility checks every six months will block even qualified people from coverage, while private insurance costs are skyrocketing. Lawmakers are being urged to close corporate tax loopholes, automate verification systems, and expand telehealth to cushion the blow to vulnerable Californians.
California
New York Islanders
fromwww.amny.com
2 months agoOp-Ed | As healthcare costs surge, lawmakers should focus on reforming rather than expanding costly government programs amNewYork
Expanding 340B program and rising healthcare costs are exacerbating unaffordability, harming minority-owned businesses, and lacking transparency and oversight.
Healthcare
fromLondon Business News | Londonlovesbusiness.com
2 weeks agoCovid inquiry warns UK emergency care 'struggling to cope' - London Business News | Londonlovesbusiness.com
Ongoing capacity issues in emergency care threaten the UK's healthcare system's preparedness for future pandemics, according to the Royal College of Emergency Medicine.
fromBoston.com
2 weeks agoMassachusetts ER doctors say long wait times reflect a health system under strain
For Massachusetts emergency physicians, that dream captures a simple truth: long ER waits rarely steam from care inside the department. Instead, doctors say they're the result of bottlenecks across a system stretched thin by staffing shortages, aging patients, limited hospital beds, and gaps in primary care.
Healthcare
#hospital-closure
Healthcare
fromGothamist
1 month agoJersey City is losing 1 of its 2 emergency rooms. Where will patients in crisis go?
Jersey City's Heights University Hospital will close its emergency room on March 14, reducing the city's emergency care capacity and forcing residents to travel farther for urgent medical services.
Healthcare
fromwww.theguardian.com
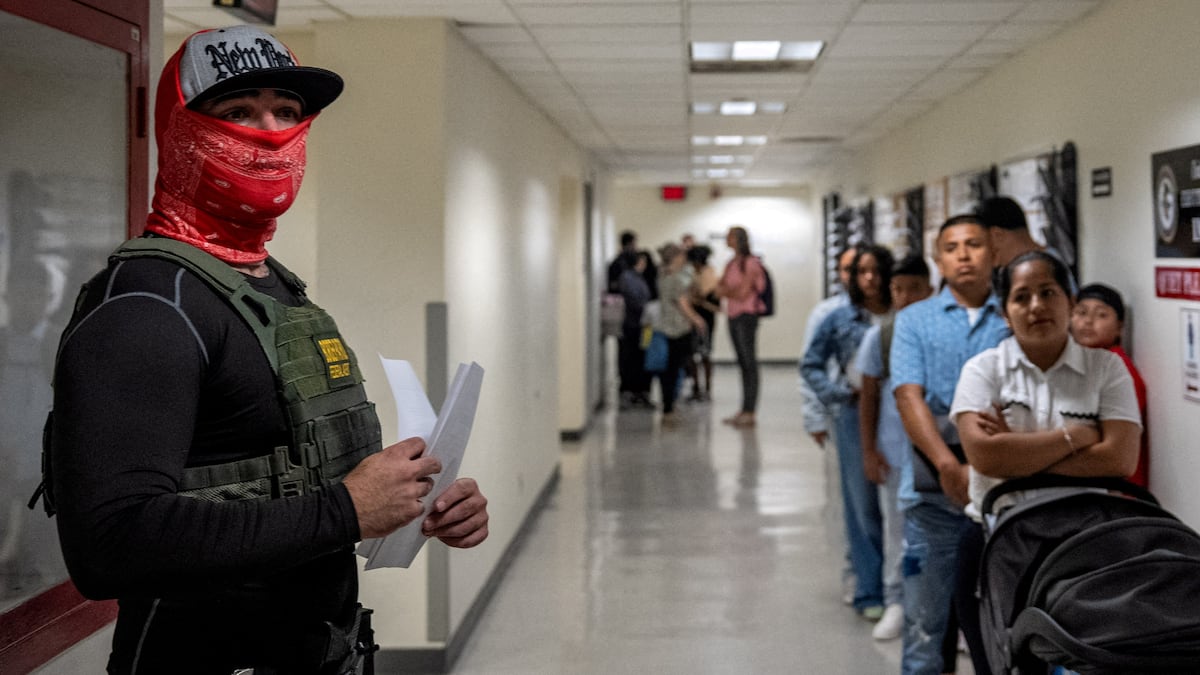
3 weeks agoThis doctor treated migrants' severe injuries at the US-Mexico wall: Political decisions made it as violent as possible'
Dr. Brian Elmore established a mobile clinic in Ciudad Juarez to provide emergency medical care to migrants facing severe injuries and limited healthcare access near the US-Mexico border.
Public health
fromBronx Times
1 month agoOUR FORGOTTEN BOROUGH | Health care in the Bronx is a dangerous game of hurry up and wait - Bronx Times
The Bronx faces a severe health-care crisis: understaffed hospitals, slow EMS response times, poor hospital rankings, and nurse strikes threaten patient care.
fromwww.sandiegouniontribune.com
2 months agoCalifornia providers brace for Medi-Cal cuts. We may not be able to serve everybody.'
The most significant immediate change arrived Jan. 1 with the expiration of enhanced premium tax credits, which help defray the cost of monthly premiums for Americans enrolled in plans sold by health insurance exchanges such as Covered California. RELATED: Bay Area Affordable Care Act policyholders brace for price hikes With Congress not renewing these subsidies, which arrived in 2021 and are in addition to the initial income-based credits made available under the Affordable Care Act, enrollees will see their payments increase significantly this year.
Public health
Healthcare
fromwww.npr.org
1 month agoIn lawsuit, Minnesota accuses Trump administration of 'weaponizing' Medicaid funding
Minnesota sued the Trump administration for withholding approximately $250 million in federal Medicaid matching funds, alleging political punishment amid fraud investigation claims.
fromLondon Business News | Londonlovesbusiness.com
1 month agoRCEM warns 'the wheels have come off' as A&Es are swamped with patients needing beds - London Business News | Londonlovesbusiness.com
All of last year, and long before, we have demanded action to ensure our hospital system is ready for when demand for Emergency Departments would spike. This did not happen, we found ourselves in a particularly busy winter and now the wheels have come off. Demand spikes in the colder months; it always does. It cannot, should not, be the case that we have to pray for a quiet January for fear the system won't cope. We should simply plan for a normal one.
Public health
Healthcare
fromBusiness Insider
1 month agoWaiting for Medicare and skipping prescriptions: Meet the Americans on the brink of losing health insurance
Expiration of enhanced ACA subsidies on December 31 caused monthly premiums to spike hundreds of dollars, forcing over 1 million Americans to cancel marketplace plans between early 2025 and 2026.
Healthcare
fromGothamist
1 month agoER at troubled hospital in Jersey City's Heights gets a lifeline, for two weeks
Heights University Hospital's emergency department will remain open through March 14 after initially planning to close, but city and state officials say this two-week extension is insufficient for the Heights neighborhood.
fromBusiness Insider
2 months agoWe want to hear your story about healthcare access
In 2026, the US healthcare system is changing. Enhanced Affordable Care Act subsidies have expired, causing premiums for marketplace plans to spike - and pricing some families out of health insurance entirely. President Donald Trump's One Big Beautiful Bill Act will reduce coverage for some patients with Medicaid and funding for hospitals, especially those in rural areas. Costs for Medicare and private insurance are also rising: Employer-based healthcare premiums have increased by 9%, the largest rise in more than a decade.
Healthcare
fromBoston.com
1 month agoMassachusetts emergency room wait times rank among the longest in the U.S.
If you find yourself in need of emergency care in Massachusetts, it could take a while. The Bay State ranks No. 3 in the U.S. for longest average time patients spend in the emergency department, according to World Population Review. Patients here spend an average of 189 minutes - more than three hours - in the ER before leaving the hospital. Only Maryland (228 minutes) and Delaware (195 minutes) report longer average delays.
Healthcare
Healthcare
fromLos Angeles Times
1 month agoA California county's only hospital cleared a federal hurdle, but it still needs millions to reopen
A new federal law restores Glenn Medical Center's critical access designation, enabling full Medicare reimbursement but not funding the estimated $40–50 million needed to reopen.
[ Load more ]